

The mind-body experience and the future for psychiatry
- Tamara Searle

- Aug 21, 2020
- 7 min read
Updated: Mar 23, 2023
Special note from the editors: This is the second blog of our new series, The future of mental health as seen by the future leaders in mental health, written by the 2020 ‘Psych Stars.’ Selected by The Royal College of Psychiatrists, Psych Star ambassadors are a group of final year medical students awarded for their particular interest and commitment to psychiatry. During the year-long scheme as Psych Stars, students are nurtured in their interest in psychiatry through the assignment of mentors, by gaining access to learning resources and events, and by becoming part of a network of like-minded students. More information on the Psych Stars scheme can be read here. We have decided to invite each of the Psych Stars to write a blog on how they envision the future of mental health by choosing an area in which they are passionate. We have decided to run the series as a celebration of these student’s success and to provide an outlook for each of the awardees to share their passion. With a new blog published each Friday, the series will run over the next few months.
As a final year medical student, I have been exposed to a wide range of medical and surgical specialities. I have noticed, in almost every placement I have attended, that patients with long-standing acute and chronic conditions often face a barrage of mental health issues on top of their physical ill-health.
This often seemed to be unrecognised by both the patient and the treating physician.
Mental health services are organised into mental health trusts which are managerially separate from general hospitals even if they are on the same geographical site. This has meant that psychiatrists tend not to work closely with other specialities and Liaison psychiatry services — which specialises in the interface between general medicine and psychiatry — are not always able to fill this void.

Patients with chronic health conditions are more likely to suffer from mental health issues and patients with mental health problems are more likely to experience physical ill-health. Recognising this and addressing it openly would lead to benefits for patients whose health concerns would be addressed in a more holistic way (an approach that sees the person as a whole).
There would also be benefits for the physicians, who often experience frustration that their patients’ physical health is not improving as much as expected, often because of their poor mental health.
Finally, for a parsimonious healthcare system, the benefit of treating patients holistically means that costs of repeated attendance at hospital outpatient clinics would be reduced.
In this blog, I will discuss how joint working between physicians and psychiatrists can improve patient treatment through the discussion of two examples of mind-body interaction: the mind-gut connection and psychodermatology.
I have chosen these two areas specifically because of my experience of them from clinical placements. I was fascinated to see the impact of holistic treatment for patients with dermatological (skin) or gastroenterological (digestive system) issues.
However, many other specialities such as cardiovascular (heart) and rheumatology (joints) also have equivalent areas of mind-body interaction. Recognition of the importance of the mind-body relationship should be part of the armamentarium of all clinicians.
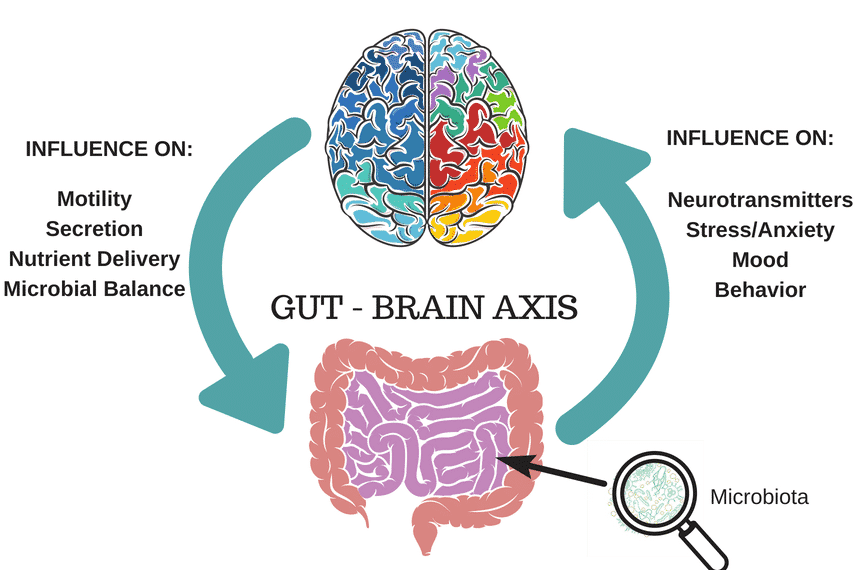
The mind-gut connection
The enteric (gastrointestinal) nervous system has long been recognised as the body’s “second brain”, with colloquial phrases such as ‘going with your gut’ or feeling ‘butterflies in your stomach’ being common parlance.
Scientific evidence has legitimised these expressions, and accumulating evidence supports the critical importance of the mind-gut interface.
Some conditions such as irritable bowel syndrome (IBS) are known to have an important psychological component. This leads many clinicians to simply dismiss their patients as having medically unexplained symptoms.
Their patients, who are suffering with painful and debilitating symptoms, are often left feeling frustrated and abandoned.
On the other hand, inflammatory bowel disease (IBD), which has an established cause, is often treated aggressively with medication by physicians. However, clinicians often fail to address the psychological sequelae of this group of diseases.
Learning to live with a chronic condition, managing to live well, and controlling the stress accompanying IBD, must not be overlooked, and is a crucial supplement to pharmacological (medicinal) and surgical treatment.
The increasing awareness of the mind-gut connection has led to the development of specialist holistic professionals. For example, as part of my clinical placement, I shadowed an IBS hypnotherapist, where talking therapy and cognitive behavioural therapy (CBT) are integrated into the treatment plan to address the psychological aspects of IBS.
This involved performing relaxation hypnotherapy exercises, as well as addressing underlying anxieties, making significant improvements in what could be a painful and incapacitating illness.
I found the impact that this therapy had on patients astounding.
Patients who had reported of debilitating chronic pain and embarrassment were able to have normal lives as a result of this therapy after only a few months.
Patients who had refused to leave the house for fear of not reaching the toilet in time felt significantly less anxious with almost no symptoms after a few months of hypnotherapy.
Peter Whorwell, Professor of Medicine and Gastroenterology at the University of Manchester, has been exploring the use of hypnotherapy in IBS for forty years. His research has highlighted that more than 60% of IBS patients who have hypnotherapy are able to see significant and maintainable long-term improvements in their symptoms. The National Institute for Clinical and Care Excellence now lists hypnotherapy as one of the treatments for IBS.
However, this is not widely available on the National Health Service. Greater awareness of its possible applications in improving the quality of life patients with IBS and IBD is warranted.
Other psychological therapies include psychotherapy, CBT, interpersonal therapy, relaxation therapy and stress management. Systematic reviews have found that CBT, multicomponent psychological therapy, dynamic psychotherapy and interpersonal therapy may be particularly useful for these patients. Higher-quality studies are required to support the use of these treatments.

Psychodermatology
In this second experience, the psychiatric component was also made abundantly clear to me.
In my dermatology placement, I was astounded to learn that 30 to 60 percent of patients with common, chronic skin conditions, such as psoriasis or eczema, also suffer from significant mental health problems.
This shocking statistic has resulted in the development of much-needed psychodermatology clinics. Various models for these clinics have been set up.
In the clinic I attended during my psychiatry placement, patients were seen by a consultant dermatologist and either a psychologist or a psychiatrist together in the clinic, and then separately by a psychologist when appropriate.
Patients who had suffered from lifelong eczema or psoriasis spoke of their reluctance and anxiety at leaving the house, and the depression and suicidal thoughts with which they were plagued. The hour-long appointments provided patients with the opportunity to seek treatment beyond pharmacological therapy for their skin condition, something impossible in a rushed ten-minute slot in an overbooked dermatology clinic.

Patients received CBT with the psychologist to help manage their symptoms and their anxiety, and medications, such as anti-depressants, where indicated. These kinds of treatments could lead to improvement in the patients’ skin conditions as well as their mental health and wellbeing.
I also saw patients presenting at the psychodermatology clinic who had severe psychiatric disorders relating to beliefs about their skin.
Several patients I saw suffered from delusional parasitosis (Ekbom’s syndrome) in which they held the unshakable belief that their bodies were infested with lice and fleas. The following patients described are compilations of stories and not real patients, so that they are not identifiable.
One patient had excoriations all over his body and refused to leave the house for fear of what people might think of him. The dermatologist listened and acknowledged the patient’s concerns whilst the psychiatrist was able to find the medical cause of this itching. This was due to an underactive thyroid, meaning that he had low levels of thyroid hormone responsible for regulating his metabolism. This can lead to reduced sweating and subsequent itching as in this example. This is an example of a collaborative working relationship to develop to ensure the best possible outcome for the patient.
An elderly patient believed that pigeons were inhabiting his house and causing fleas to infest his body. He demanded investigations and spent hours on internet chat rooms discussing his symptoms. He even presented a “photo” of one of the supposed fleas. His main fears were about infecting other people with whom he lived or worked. The psychiatrist was able to prescribe risperidone, an antipsychotic medication, for this patient, whilst the dermatologist reassured the patient that there was no infestation. By working together in this way, the patient accepted prescription of an anti-psychotic medication when it would have been highly unlikely that the patient would have agreed to see a psychiatrist in the normal way.
Psychodermatology clinics are currently only available in three centres in the United Kingdom; further development of these services are urgently needed across the country to treat patients such as these. I found this placement so interesting that I arranged my elective placement at a psychodermatology clinic abroad, but unfortunately, this was cancelled due to COVID-19. I hope I can rearrange this placement at a future time.

Whilst psychodermatology is a very niche subspeciality, it exemplifies the immense value of psychiatrists working with other healthcare professionals across all medical specialities.
I have discussed two examples briefly from my own experiences, yet many other fields have similar interfaces. For example, rheumatologists face difficulties treating patients with fibromyalgia, whilst ear nose and throat consultants struggle to treat patients with chronic tinnitus.
In conclusion, clinicians must work together to acknowledge the mind-body relationship. This is fundamental for improving both the psychological and medical treatment of all patients.
In the future, psychiatrists must find creative ways to reach out to this subgroup of patients who otherwise might be difficult to engage. Psychiatry must become a more integrated part of patients’ holistic journey.
NOTE FROM THE EDITORS: If you enjoyed today’s blog by Rebecca, be sure to head over to InSPIre the Mind and check out the previous and first blog in our Psych Star series all about compassion. Stay tuned for more from these fantastic medical students every Friday!


