

Seeing What Isn’t There: Visual Hallucinations In Parkinson’s
- Miriam Vignando

- Mar 11
- 5 min read

Parkinson’s disease is a neurodegenerative disorder primarily known for its motor symptoms. However, a substantial proportion of people living with Parkinson’s have a wide range of non-motor symptoms, among which visual hallucinations are very frequent. Approximately 60% of patients are estimated to develop this symptom within 12 years of diagnosis.
Dementia can be defined as a decline of thinking skills (e.g., memory, language) that significantly interferes with daily life. As a progressive disease, symptoms worsen over time. While we often associate this with other diseases like Alzheimer’s, dementia in Parkinson’s disease is both serious and costly with an approximate prevalence of 20-40%.
People with Parkinson’s disease may have a steeper cognitive decline, which may be a possible early marker and treatment target that might also have beneficial effects on other serious symptoms later. However, we still don’t exactly know whether or why hallucinations and this cognitive impairment share the same causes. No treatment for hallucinations in this disease is yet showing the required efficacy and specificity. Neuroscience research is seeing slow but meaningful progress towards the discovery of disease-modifying drugs for dementia and hallucinations in Parkinson’s. This could provide a window into some of the mechanisms associated with an accelerated decline.
I am an Alzheimer’s Research UK Research Fellow at King’s College London. My research hopes to uncover the reasons why some people are more likely to develop dementia faster than others when they have the same diagnosis. Among my main research interests is Parkinson’s disease, and during my previous postdoc I have had the opportunity to work on a project on Parkinson’s disease psychosis led by Prof. Mitul Mehta; research that inspired my interest in hallucinations in Parkinson’s disease.
The Hallucinations Continuum in Parkinson’s
Hallucinations are defined as perceptual experiences that happen without a sensory stimulus, for example, seeing something that is not there. In Parkinson’s, hallucinations typically begin as what we call ‘minor hallucinations’. These include, for example, feeling a presence in the room, seeing movement at the edge of the visual field, or as visual illusions (i.e., seeing faces or animals in patterns, not unlike the famous face in the toasted bread phenomenon). These early hallucinations are thought to be linked to problems in brainstem systems (in violet in the image below) that help control eye movements and to pathways in the brain that process visual motion. Then, as the disease progresses, some develop fully formed visual hallucinations, often involving persons, faces, and animals. These are thought to reflect dysfunction in a wider network of brain regions (shaded in blue).

What are the parts of the brain involved in VH?
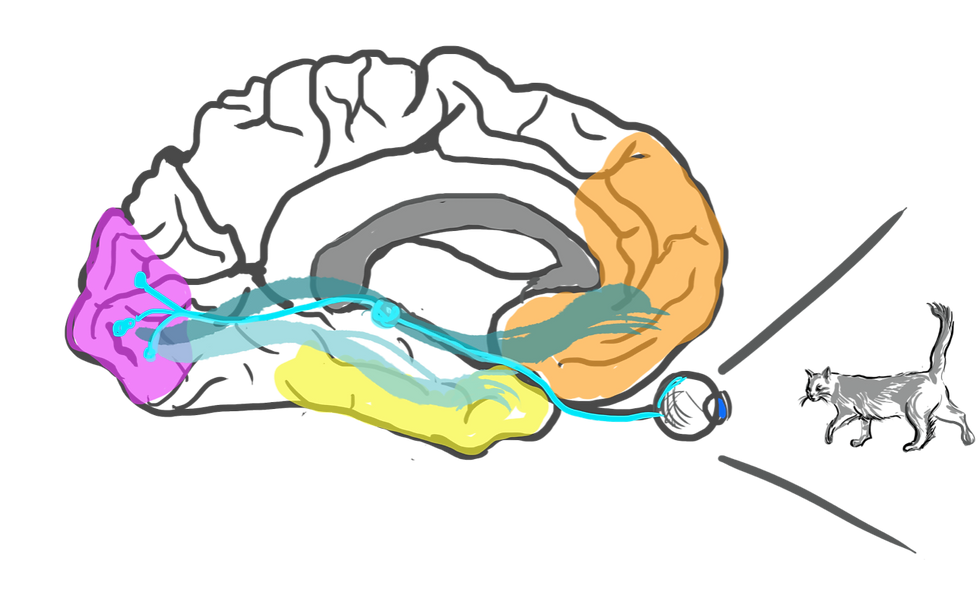
Visual information is transmitted from the retina in the eye to the primary visual cortex (in pink in the next figure below), a region of the brain crucial in processing visual stimuli. This region then communicates with inferior temporal regions (yellow) and the prefrontal cortex (orange). All these regions together are part of an object recognition network whereby all the components work together to identify objects, picking out from our memory storage what object corresponds to the characteristics of the image we are seeing. For example, if it is small, moves, has 4 legs, whiskers, and pointy ears, we can deduce that it is very likely to be a cat.
However, we need to keep in mind that our brain is always performing a kind of guesswork when we are going about our lives and scanning the environment. We always interpret our environment considering our prior experiences and contextual information, both sensory but also emotional and situational. So, while we would generally discount any shadow or shape while navigating a dark environment as a bush or a tree, if we happen to find ourselves in such a situation after, for example, having recently watched a horror movie, we might be biased and primed to believe there is something there that isn’t. This happens because we need both sensory information and prior beliefs to make our predictions about the world. If there is a combination of a weak sensory input with very strong beliefs, we might experience something that is akin to a visual hallucination. In Parkinson’s, due to the complex neurology associated to it, this can happen more frequently.
The brain in Parkinson’s disease is affected by multiple interacting changes. One pathological hallmark is the abnormal accumulation of alpha-synuclein, a protein that can “misfold” (fail to adopt its correct shape) and gather abnormally in the brain; this in turn can cause the motor symptoms we typically see in this disease. This “altered balance” is complicated by the interaction of this pathology with other chemicals in the brain, such as dopamine (linked to mood and reward, but also movement), serotonin (involved in hallucinations, but also mood), and acetylcholine (important for cognition).

What did we discover so far?
My work in the past few years builds on these foundations and has revolved around understanding the brain mechanisms behind visual hallucinations in Parkinson’s. First, we pooled together data from different research centres, finding differences in brain structure in people with Parkinson’s with hallucinations despite having a similar profile to those without in parts of the brain that include the regions involved in visual processing and recognition (including the brain regions shown in Figure 2). Then we examined functional signatures of hallucinations using electroencephalography (EEG). EEG non-invasively measures brain waves by using electrodes placed on the scalp. We used a simple task that has proven reliable in psychosis research to investigate the mechanism with which we use sensory information and prior experience to make predictions.

We used a version of the task adapted for vision, but it can be used with sound stimuli too. The task requires participants to make a judgement about the changes in size of a cross at the centre of the screen, while the peripheral stimuli (black bars on both sides of the screen) keep appearing in the same orientation. When these bars appear in a slightly different orientation, the brain catches up with this change, even if it’s something we don’t notice. People with schizophrenia show a very reduced response to this change. We found that people with Parkinson’s with hallucinations had a reduced response to this task. We were able to confirm that we can use this task as a strong marker for psychosis in Parkinson’s disease. This is important because the experience of individuals living with Parkinson’s varies greatly and a deeper knowledge of the brain mechanisms involved in hallucinations and psychosis can help individuals better understand the symptoms they are experiencing.
The next step to truly understand the relationship of hallucinations and cognition in Parkinson’s would be to examine how these results can be validated by following people over the years. By understanding why hallucinations happen in Parkinson’s, we may be able to identify earlier markers of progression and thus develop more precise treatments for both psychosis and cognitive decline.


